Delivery
What is delivery ?
Childbirth (also called labor, birth, partus or parturition) is the culmination of a human pregnancy or gestation period with the expulsion of one or more newborn infants from a woman's uterus. The process of normal human childbirth is categorized in three stages of labour: the shortening and dilation of the cervix, descent and birth of the infant, and birth of the placenta. In many cases, with increasing frequency, childbirth is achieved through caesarean section, the removal of the neonate through a surgical incision in the abdomen, rather than through vaginal birth
Signs
Labor is sometimes accompanied by intense and prolonged pain. Pain levels reported by laboring women vary widely. Pain levels appear to be influenced by fear and anxiety levels. Some other factors may include experience with prior childbirth, age, ethnicity, preparation, physical environment and immobility.
Psychological
Childbirth can be an intense event and strong emotions, both positive and negative, can be brought to the surface.
Between 70% and 80% of mothers in the United States report some feelings of sadness or "baby blues" after childbirth. Postpartum depression may develop in some women; about 10% of mothers in the United States are diagnosed with this condition. Abnormal and persistent fear of childbirth is known as tokophobia.
Preventive group therapy has proven effective as a prophylactic treatment for postpartum depression.
Childbirth is stressful for the infant. In addition to the normal stress of leaving the protected uterine environment, additional stresses associated with breech birth, such as asphyxiation, may affect the infant's brain
Normal human birth
Vaginal birth
Because humans are bipedal with an erect stance and have, in relation to the size of the pelvis, the biggest head of any mammalian species, human fetuses and human female pelvises are adapted to make birth possible.
The erect posture causes the weight of the abdominal contents to thrust on the pelvic floor, a complex structure which must not only support this weight but allow three channels to pass through it: the urethra, the vagina and the rectum. The head and shoulders require a specific sequence of maneuvers to occur for the bony head and shoulders to pass through the bony ring of the pelvis.
Six phases:
- Engagement of the fetal head in the transverse position. The baby's head is facing across the pelvis at one or other of the mother's hips.
- Descent and flexion of the fetal head.
- Internal rotation. The fetal head rotates 90 degrees to the occipito-anterior position so that the baby's face is towards the mother's rectum.
- Delivery by extension. The fetal head passes out of the birth canal. Its head is tilted forwards so that the crown of its head leads the way through the vagina.
- Restitution. The fetal head turns through 45 degrees to restore its normal relationship with the shoulders, which are still at an angle.
- External rotation. The shoulders repeat the corkscrew movements of the head, which can be seen in the final movements of the fetal head.
The fetal head may temporarily change shape substantially (becoming more elongated) as it moves through the birth canal. This change in the shape of the fetal head is called molding and is much more prominent in women having their first vaginal delivery.
Latent phase
The latent phase of labor, also called prodromal labor, and the contractions may be an intensification of the Braxton Hicks contractions that may start around 26 weeks gestation. Cervical effacement occurs during the closing weeks of pregnancy and is usually complete or near complete, by the end of the latent phase. Cervical effacement or cervical dilation is the thinning and stretching of the cervix. The degree of cervical effacement may be felt during a vaginal examination but is not necessary. A 'long' cervix implies that not much has been taken into the lower segment, and vice versa for a 'short' cervix. Latent phase ends with the onset of active first stage; when the cervix is about 4 cm dilated.
First stage: dilation
There are several factors that midwives and physicians use to assess the laboring mother's progress, and these are defined by the Bishop Score. The Bishop score is also used as a means to predict whether the mother is likely to spontaneously progress into second stage (delivery).
The first stage of labor starts classically when the effaced (thinned) cervix is 3 cm dilated. There is a variation in this point as some women may or may not have active contractions prior to reaching this point. The onset of actual labor is defined when the cervix begins to progressively dilate. Rupture of the membranes, or a blood stained 'show' may or may not occur at or around this stage.
Uterine muscles form opposing spirals from the top of the upper segment of the uterus to its junction with the lower segment. During effacement, the cervix becomes incorporated into the lower segment of the uterus. During a contraction, these muscles contract causing shortening of the upper segment and drawing upwards of the lower segment, in a gradual expulsive motion. The presenting fetal part then is permitted to descend. Full dilation is reached when the cervix has widened enough to allow passage of the baby's head, around 10 cm dilation for a term baby.
The duration of labour varies widely, but active phase averages some 20 hours for women giving birth to their first child ("primiparae") and 8 hours for women who have already given birth ("multiparae"). Active phase arrest is defined as in a primigravid woman as the failure of the cervix to dilate at a rate of 1.2 cm/hr over a period of at least two hours. This definition is based on Friedman's Curve, which plots the typical rate of cervical dilation and fetal descent during active labor. Some practitioners may diagnose "Failure to Progress", and consequently, perform a Cesarean
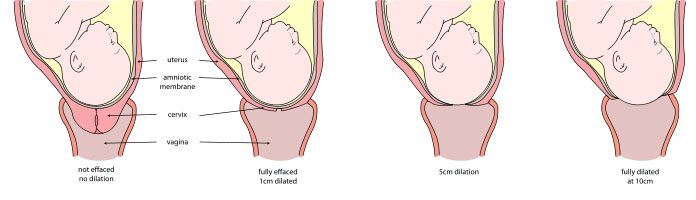
Sequence of cervix dilation during labor
This stage begins when the cervix is fully dilated, and ends when the baby is born. As pressure on the cervix increases, the Ferguson reflex increases uterine contractions so that the second stage can go ahead. At the beginning of the normal second stage, the head is fully engaged in the pelvis; the widest diameter of the head has passed below the level of the pelvic inlet. The fetal head then continues descent into the pelvis, below the pubic arch and out through the vaginal introitus. This is assisted by the additional maternal efforts of "bearing down" or pushing. The fetal head is seen to 'crown' as the labia part. At this point, the woman may feel a burning or stinging sensation. Complete expulsion of the baby signals the successful completion of the second stage of labor.

A newborn baby with umbilical cord ready to be clamped
Breastfeeding during and after the third stage, the placenta is visible in the bowl to the right.
The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor.
The umbilical cord is routinely clamped and cut in this stage, but it would normally close naturally even if not clamped. A 2008 Cochrane Review looked into the timing of clamping the umbilical cord. It found that the time of clamping made no difference to the mother, but did have effects for the baby. If the cord is clamped after 1–3 minutes, the infant receives increased amounts of haemoglobin in their first months of life, but may have an increased risk of needing phototherapy to treat jaundice. Sometimes a newborn’s liver is slow to break down all of the red cells they had in the womb, particularly if they are left with more fetal blood from delayed cord clamping and phototherapy helps to speed the breakdown.
Placental expulsion begins as a physiological separation from the wall of the uterus. The period from just after the fetus is expelled until just after the placenta is expelled is called the third stage of labor. The average time from delivery of the baby until complete expulsion of the placenta is estimated to be 10-12 minutes dependent on whether active or expectant management is employed.
Placental expulsion can be managed actively, by giving a uterotonic such as oxytocin along with appropriate cord traction and fundal massage to assist in delivering the placenta by a skilled birth attendant. Alternatively, it can be managed expectantly, allowing the placenta to be expelled without medical assistance. In a joint statement, World Health Organization, the International Federation of Gynaecologists and Obstetricians and the International Confederations of Midwives recommend active management of the third stage in all vaginal deliveries. This is a strong recommendation of the World Health Organization backed by moderate base evidence citing reduced risk of postpartum bleeding (i.e.: obstetric hemorrhage).
In as many as 3% of all vaginal deliveries, the duration of the third stage is longer than 30 minutes and raises concern for retained placenta.
When the amniotic sac has not ruptured during labour or pushing, the infant can be born with the membranes intact. This is referred to as "being born in the caul." The caul is harmless and its membranes are easily broken and wiped away. With the advent of modern interventive obstetrics, artificial rupture of the membranes has become common, so babies are rarely born in the caul.
Fourth stage
The "fourth stage of labor" is a term used in two different senses:
- It can refer to the immediate puerperium, or the hours immediately after delivery of the placenta.
- It can be used in a more metaphorical sense to describe the weeks following delivery.
Station
Refers to the relationship of the fetal presenting part to the level of the ischial spines. When the presenting part is at the ichial spines the station is 0 (synonymous with engagement). If the presenting fetal part is above the spines, the distance is measured and described as minus stations, which range from -1 to -4 cm. If the presenting part is below the ischial spines, the distance is stated as plus stations ( +1 to +4 cm). At +3 and +4 the presenting part is at the perineum and can be seen.
Management
Eating or drinking during labor is an area of ongoing debate. While some have argued that eating in labor has no harmful effects on outcomes, others continue to have concern regarding the increased possibility of an aspiration event (choking on recently eaten foods) in the event of an emergency delivery due to the increased relaxation of the esophagus in pregnancy, upward pressure of the uterus on the stomach, and the possibility of general anesthetic in the event of an emergency cesarean.
Pain control
Non pharmaceutical
Some women prefer to avoid analgesic medication during childbirth. They can still try to alleviate labor pain using psychological preparation, education, massage, acupuncture, TENS unit use, hypnosis, or water therapy in a tub or shower. Some women like to have someone to support them during labor and birth, such as the father of the baby, a family member, a close friend, a partner, or a doula. Some women deliver in a squatting or crawling position in order to more effectively push during the second stage and so that gravity can aid the descent of the baby through the birth canal.
The human body also has a chemical response to pain, by releasing endorphins. Endorphins are present before, during, and immediately after childbirth. Some homebirth advocates believe that this hormone can induce feelings of pleasure and euphoria during childbirth,reducing the risk of maternal depression some weeks later.
Water birth is an option chosen by some women for pain relief during labor and childbirth, and some studies have shown waterbirth in an uncomplicated pregnancy to reduce the need for analgesia, without evidence of increased risk to mother or newborn. Hot water tubs are available in many hospitals and birthing centres.
Meditation and mind medicine techniques are also used for pain control during labour and delivery. These techniques are used in conjunction with progressive muscle relaxation and many other forms of relaxation for the mind and body to aid in pain control for women during childbirth. One such technique is the use of hypnosis in childbirth. There are a number of organizations that teach women and their partners to use a variety of techniques to assist with labor comfort, without the use of pharmaceuticals.
A new mode of analgesia is sterile water injection placed just underneath the skin in the most painful spots during labor. A control trial in Iran of 0.5mL injections was conducted with normal saline which revealed a statistical superiority with water over saline.
Pharmaceutical
Different measures for pain control have varying degrees of success and side effects to the woman and her baby. In some countries of Europe, doctors commonly prescribe inhaled nitrous oxide gas for pain control, especially as 50% nitrous oxide, 50% oxygen, known as Entonox; in the UK, midwives may use this gas without a doctor's prescription. Pethidine (with or without promethazine) may be used early in labour, as well as other opioids such as fentanyl, but if given too close to birth there is a risk of respiratory depression in the infant.
Popular medical pain control in hospitals include the regional anesthetics epidural blocks, and spinal anaesthesia. Epidural analgesia is a generally safe and effective method of relieving pain in labour, but is associated with longer labour, more operative intervention (particularly instrument delivery), and increases in cost. Generally, pain and cortisol increased throughout labor in women without EDA. Pain and stress hormones rise throughout labor for women without epidurals, while pain, fear, and stress hormones decrease upon administration of epidural analgesia, but may rise again later. Medicine administered via epidural can cross the placenta and enter the bloodstream of the fetus. Epidural analgesia has no statistically significant impact on the risk of caesarean section, and does not appear to have an immediate effect on neonatal status as determined by Apgar scores.
Augmentation
Augmentation is the process of facilitating further labour. Oxytocin has been used to increase the rate of vaginal delivery in those with a slow progress of labor.
Instrumental delivery
Obstetric forceps or ventouse may be used to facilitate childbirth.
Multiple births
In cases of a cephalic presenting twin (first baby head down), twins can often delivered vaginally. In some cases twin delivery is done in a larger delivery room or in an operating theatre, in the event of complication e.g.
- Both twins born vaginally - this can occur both presented head first or where one comes head first and the other is breech and/or helped by a forceps/ventouse delivery
- One twin born vaginally and the other by caesarean section.
- If the twins are joined at any part of the body - called conjoined twins, delivery is mostly by caesarean section.